
The impact of obese deceased donor on outcome in simultaneous pancreas/kidney transplants - A registry analysis
Angelika C. Gruessner1, Subodh J. Saggi1, Rainer WG Gruessner1.
1Medicine, SUNY Downstate Medical Center, Brooklyn, NY, United States
Introduction: The obesity epidemic is contributing to the shortage of organs available for transplantation. The (arbitrary) BMI cut points are set because the obese donor may be pre-diabetic and therefore may not be an appropriate pancreas donor. The goal of this study was to assess the risk of using an obese deceased donor for a SPK transplant.
Material: All 6,859 deceased adult donors (1/2010 - 12/2020) for a SPK with available weight data at time of transplant were analyzed. The donor BMI was classified according to WHO recommendations as ‘Underweight’, ‘Normal’, ‘Overweight’, ‘Obese Class 1’, and ‘Obese Class 2 and 3’ (See Table 1). Comprehensive description of characteristics was given. Univariate patient and graft survival rates were computed, and multifactorial models were developed to assess the risk of obesity on technical failure and long-term graft outcomes.
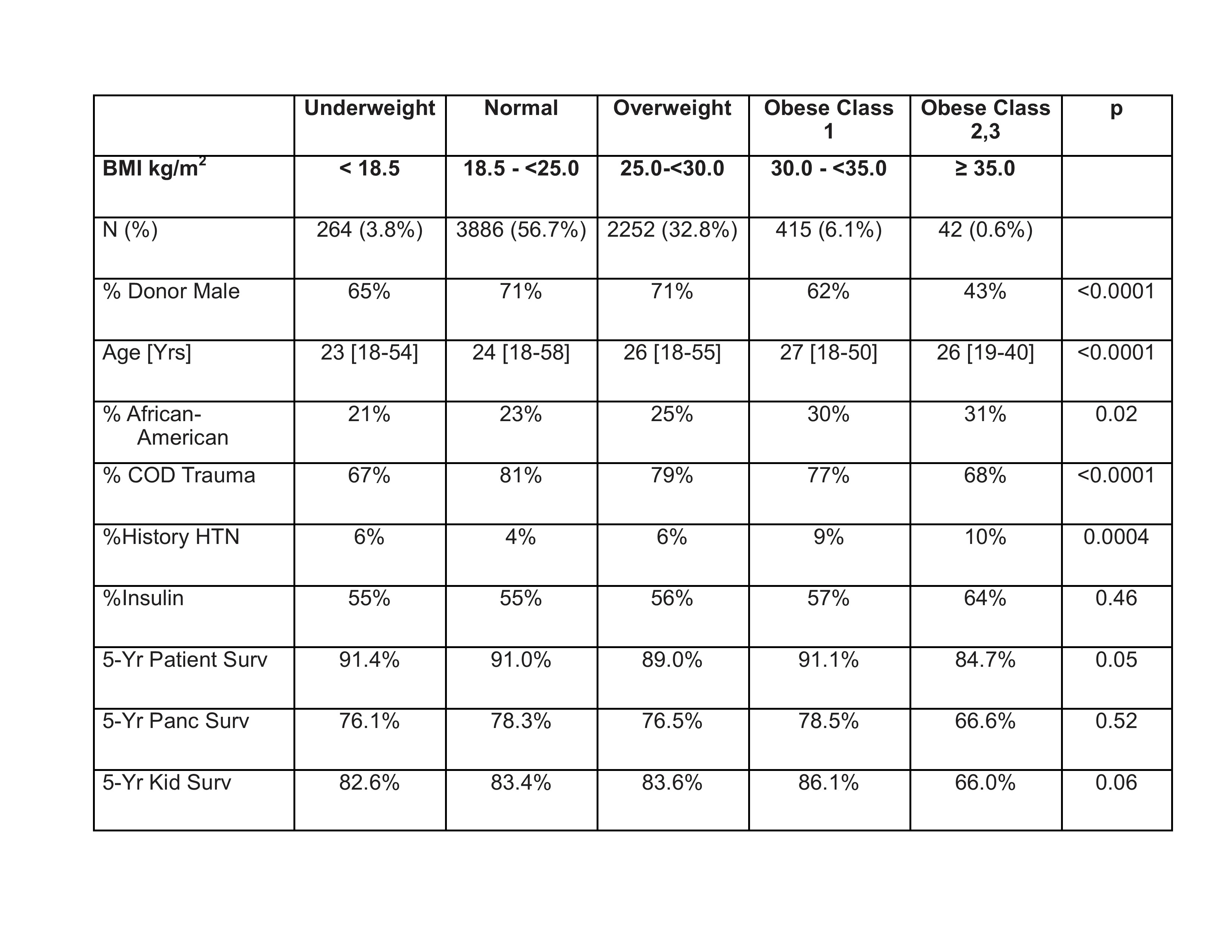
Results: Table 1 shows the different donor characteristics by BMI category. With increasing BMI there was a significant trend towards a decrease in donor age and an increase in the rate of African Americans donors. There was also an increase in female donors with increasing BMI. Univariate analysis patient survival was not negatively impacted by donor BMI for the first 4 BMI categories including Obese class 1 category donors.
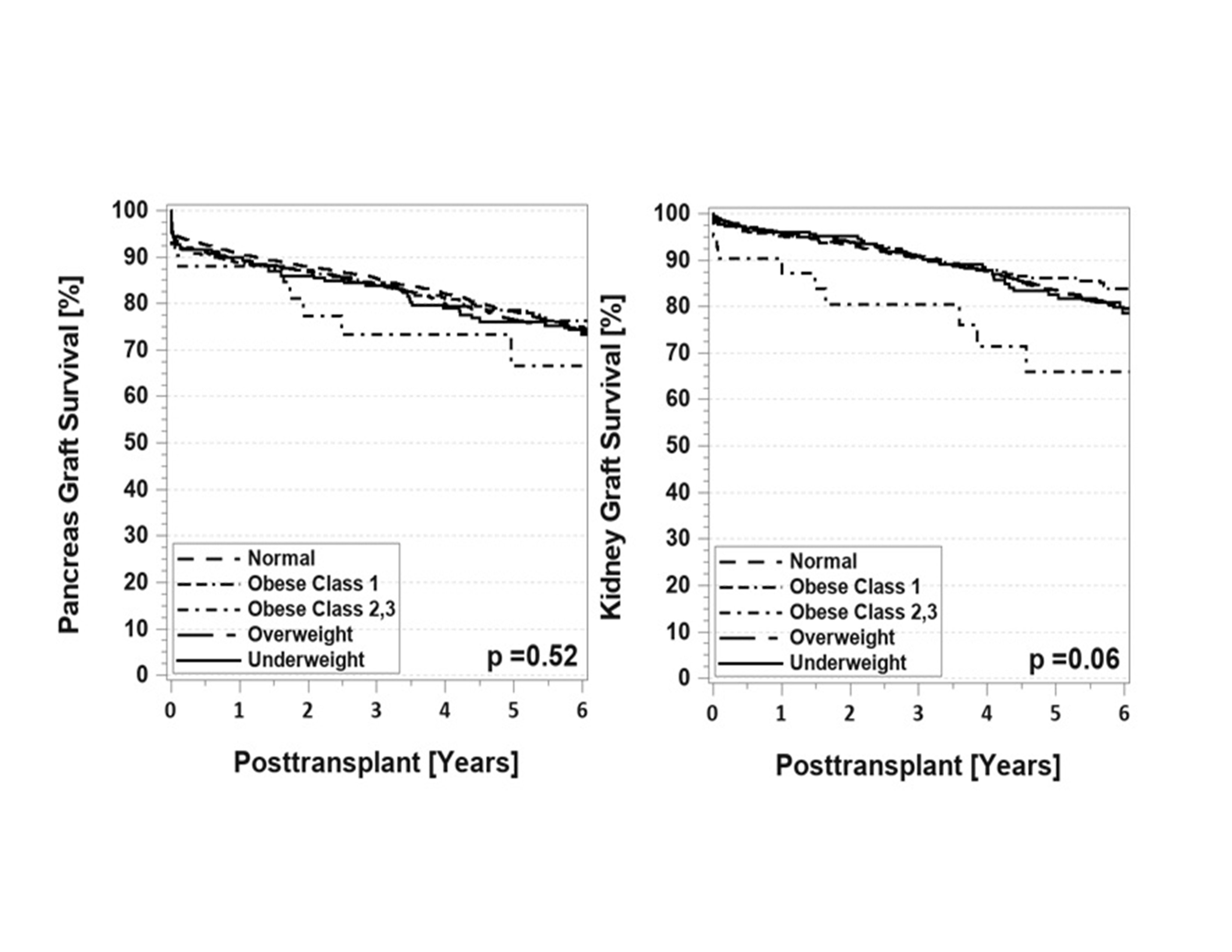
Only Obese class 2 and 3 donors had lower patient survival (Table 1). The same trend was noted for pancreas and kidney graft survival (Figure 1). The negative impact of a very high donor BMI was more evident in the kidney (vs. pancreas) graft. The multivariable adjusted Cox regression showed a relative risk for pancreas graft failure in Obese class 2 and 3 recipients of 1.7 [0.9 – 3.2] and for kidney graft failure of 2.0 [0.8-4.3].
Conclusions: This analysis showed that that excellent patient and graft outcomes in SPK can be achieved with donors with a BMI of up to 35kg/m2. A BMI over 35kg/m2 negatively impacted specifically kidney survival long-term.