
Better long-term patient and kidney graft outcome for simultaneous pancreas/kidney (SPK) versus kidney transplant alone (KTA) recipients
Angelika C. Gruessner1, Rainer WG Gruessner1.
1Medicine, SUNY Downstate Medical Center, Brooklyn, NY, United States
Introduction: Often a kidney transplant alone rather than a simultaneous pancreas and kidney transplant (SPK) is performed in patients with insulin-dependent diabetes mellitus and end-stage renal disease. A SPK is a more complex procedure, and it requires an expert transplant team. What is the long term advantage of an SPK in comparison to a kidney transplant?
Materials: To assess long-term patient and kidney graft outcome, all 11,860 primary deceased donor (DD) and living donor (LD) KTA and SPK performed between 1994 and 2000 with a primary diagnosis of DM were included. Patients had at least 20-years of follow-up.
Results: Of 11,860 transplants , 48.9% received a DD KTA, 23.5% a LD KTA and 27.6% a SPK transplant. The characteristics of the 3 groups are different. During this time, only 4.4% of SPK, but 60.7% of DD KTA and 49.8% of LD KTA received transplants due to T2DM. In T1 and T2 diabetics, the recipient and donor age of DD KTA recipients was significantly older and the recipients of a SPK significantly younger. The rate of preemptive transplants was lower in DD KTA.
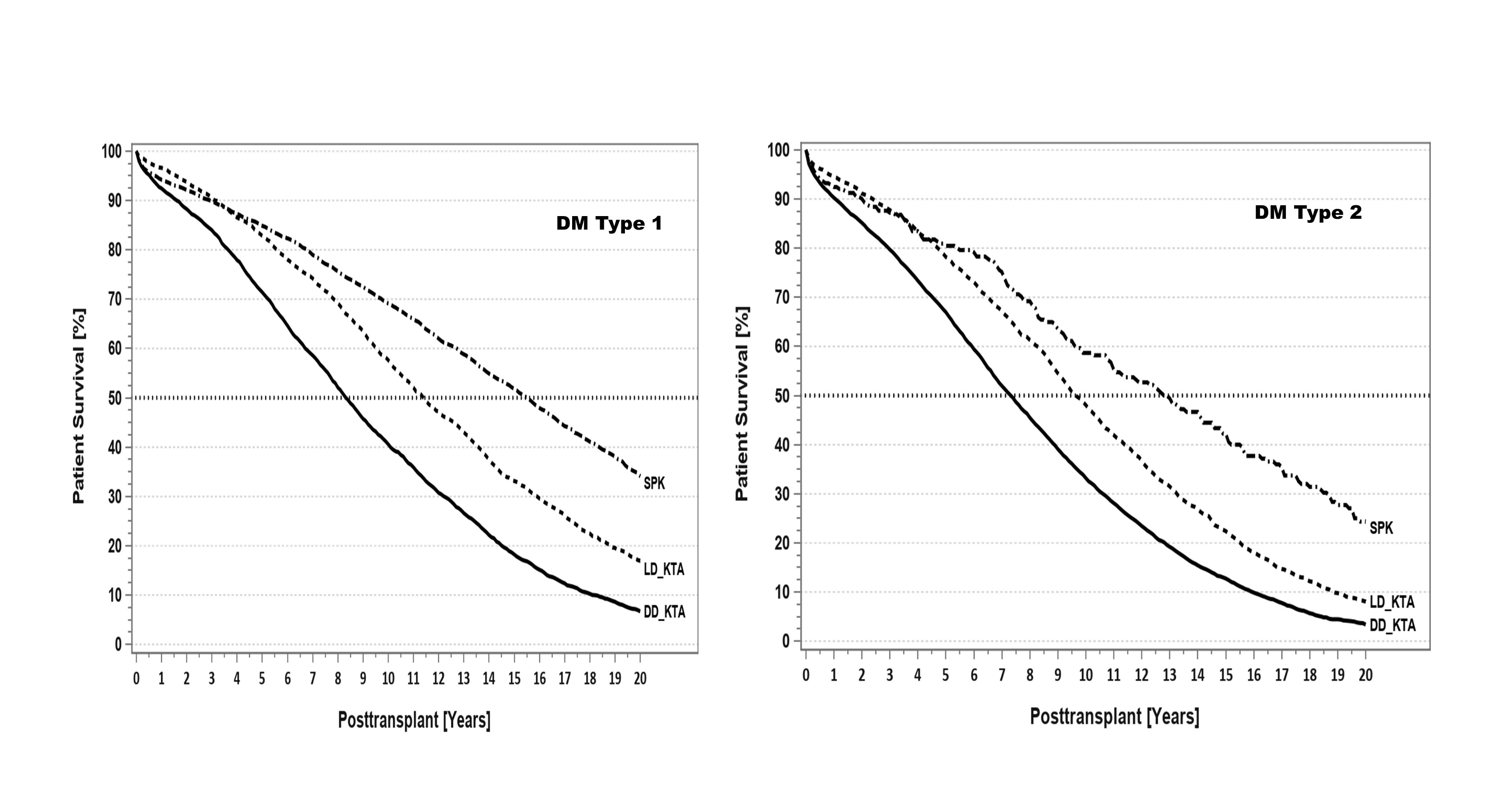
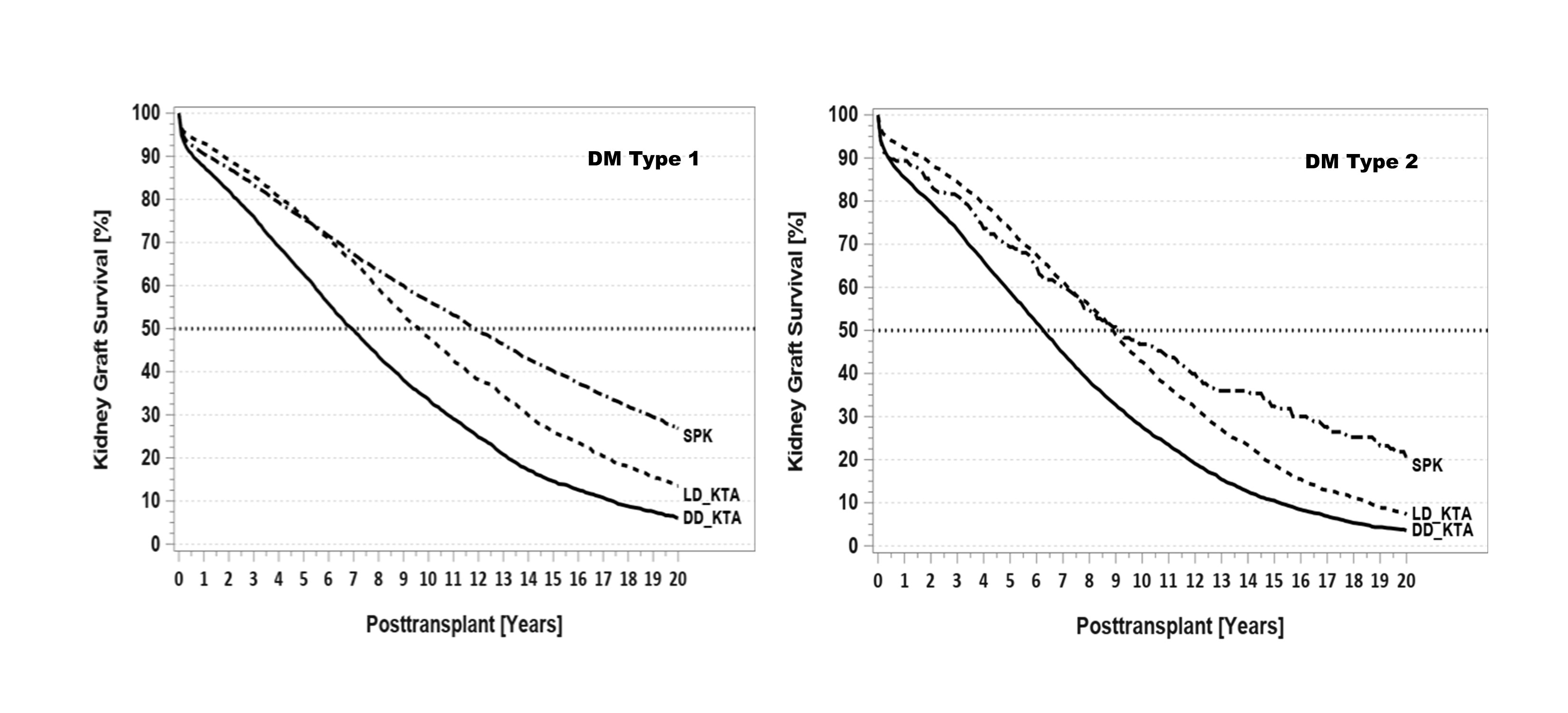
Figures 1 and 2 show univariate patient and kidney graft outcomes with a significant long-term advantage for SPK. The adjusted multivariable results showed clear long-term advantage for SPK vs. KTA. The relative risk (RR) to die was increased for DD KTA by 97%, for LD KTA by 37% when compared to SPK. The RR for long-term kidney graft failure was increased by 66% for DD KTA and 14% for LD KTA when compared to SPK. When dying with a functioning kidney graft was censored, the advantage of an SPK kidney graft was still significantly higher than for DD KTA and similar to LD KTA.
Conclusions: Due to the very heterogenous distribution of recipient and donor risk factors, any comparison of the 3 transplant types has to be analyzed very carefully. Our analysis shows significantly better long-term outcome for SPK transplants that were performed >20 years ago when compared to both LD and DD KTA.