Impact of preemptive transplantation on long-term outcomes after simultaneous pancreas-kidney transplantation
Enrique Montagud-Marrahi1,2, Alicia A. Molina-Andújar1,2, David D. Cucchiari1,2, Ignacio I. Revuelta1,2, Núria N. Esforzado1, Frederic F. Cofan1, Jessica J. Ugalde1,2, Gaston G. Piñeiro1,2, Sabina S. Ruiz4, Joana J. Ferrer3, M. Ángeles MA Garcia-Criado5, Antonio J. A. Amor4, Enric E. Esmatjes4, Constantino C. Fondevila3, Fritz F. Diekmann1,2, Pedro P. Ventura-Aguiar1,2.
1Nephrology and Kidney Transplantation Department, Hospital Clinic de Barcelona, Barcelona, Spain; 2Laboratori Experimental de Nefrologia I Trasplantament (LENIT), Fundació Clínic per a la Recerca Biomèdica (FCRB), Barcelona, Spain; 3Hepatobiliopancreatic and Liver Transplant Department, Hospital Clínic Barcelona, Barcelona, Spain; 4Diabetes Unit. Endocrinology and Nutrition Department, Hospital Clínic Barcelona, Barcelona, Spain; 5Radiology Department, Hospital Clinic de Barcelona, Barcelona, Spain
Introduction: Simultaneous Pancreas-Kidney transplantation (SPK) is an established treatment option for patients with End-Stage Kidney Disease (ESKD) and diabetes, which provides multiple benefits related to patient survival and cardiovascular risk when compared to kidney transplantation alone. Previous studies have suggested that, also in SPK, a preemptive approach is associated with a significant survival advantage when compared to non-preemptive SPK, although available information on the impact of preemptive SPK on recipient and grafts outcomes remains controversial.
Methods: we explore the influence of preemptive SPK on recipient, kidney and pancreas graft survival through a retrospective study with 9690 SPK recipients from the OPTN/UNOS database between 2000 and 2017. An Inverse probability of treatment weighting (IPTW) was used to account for covariate imbalance between preemptive and dialysis transplant recipients.
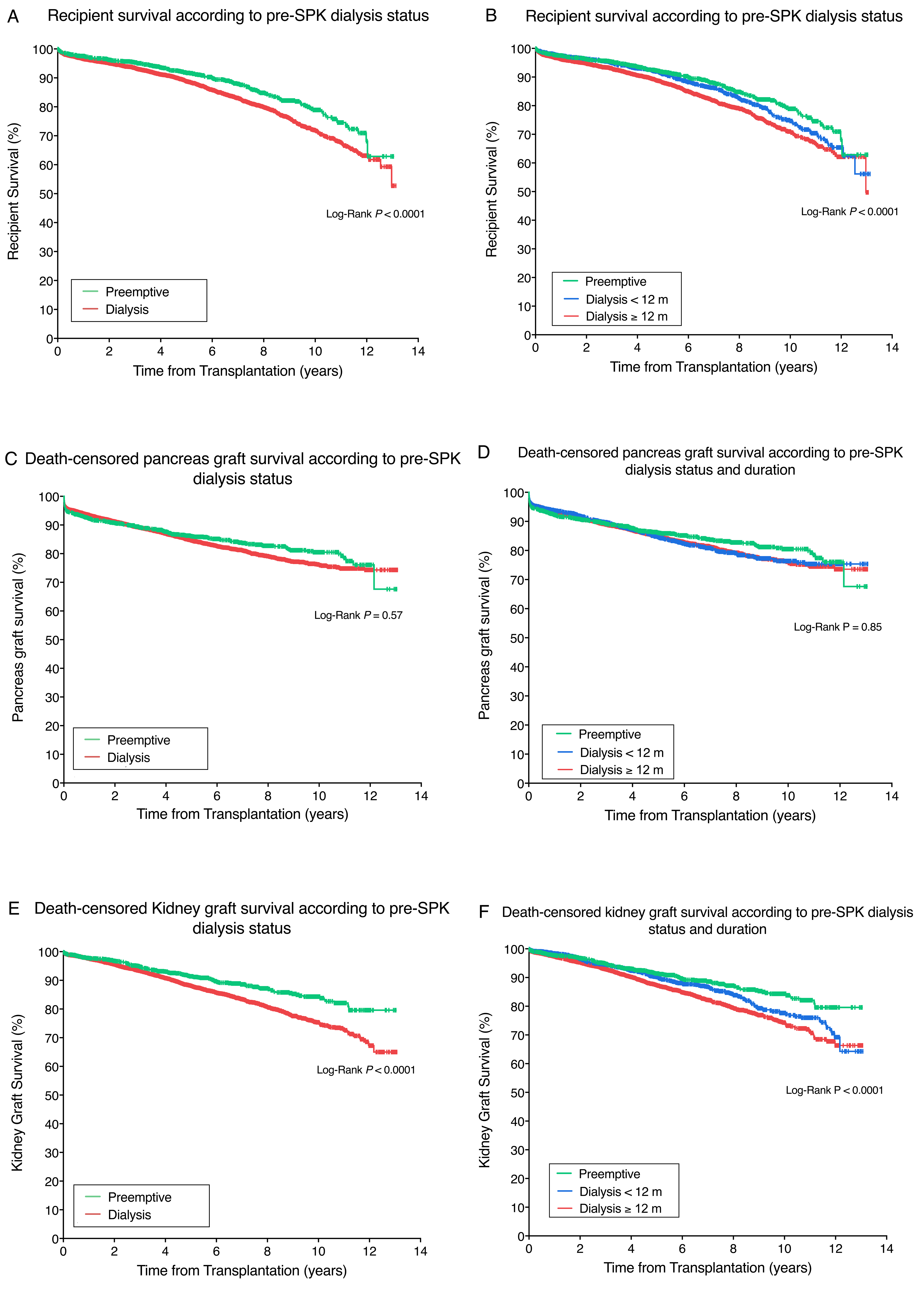
Results: A total of 1796 (19%) patients were preemptively transplanted. After inverse probability of treatment weighting, recipient (97.6%, 91.7% and 78.9% vs 96.6%, 88.8% and 71.8% at 1, 5 and 10 years for preemptive vs dialysis, respectively, P<0.0001) and death-censored kidney graft survival (97.8%, 91.4% and 84.3% vs 97.63%, 88.1% and 75.4% for the preemptive and dialysis at 1, 5 and 10 years, respectively, P<0.0001) were higher for the preemptive group. No differences were observed neither for pancreas graft survival nor patients with Type 2 Diabetes. Dialysis (HR 1.66 [95%CI 1.32-2.09], P<0.0001) and dialysis duration ≥12 months (HR 1.78 [95%CI 1.42-2.24], P< 0.0001) were associated with an increased risk of recipient death and kidney graft failure (HR 1.46 [95%CI 1.18-1.81, P<0.001 and HR 1.53 [95%CI 1.23-1.91], P<0.0001 for dialysis and dialysis duration ≥12 months, respectively).
Discussion/Conclusions: In a cohort of 9690 SPK recipients, dialysis was associated with an increased risk of recipient death and kidney graft loss of up to 66% and 46% when compared with recipients transplanted preemptively. Furthermore, this risk increased with the dialysis duration prior to the SPK. Interestingly these results were observed in T1D, but not in T2D recipients. Overall, our findings suggest that preemptive SPK is associated with a significant survival advantage for SPK recipients, thus reinforcing the need for an early referral of ESKD and diabetes patients to be evaluated as potential SPK recipients.